Article Text

Abstract
We report on the establishment of “general anaesthesia (GA) to local anaesthesia (LA) conversion" or GALA initiative at Sheffield Teaching Hospitals NHS Foundation Trust. Through GALA initiative, long waiters for cataract surgery under GA or LA with intravenous sedation were counselled for LA surgery. With careful surgical planning and personalised solutions to LA barriers, LA-converted patients reported good visual and surgical experience outcomes. The GALA initiative reduced cataract surgery waiting times of participants by 11 weeks and increased GA list capacity by three to four theatre lists in its four months of pilot run. This initiative did not limit training opportunities for ophthalmology trainees whose training was affected significantly during the pandemic.
- COVID-19
- healthcare quality improvement
- anaesthesia
- waiting lists
- surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The Royal College of Ophthalmologists (RCOphth) recommended the suspension of all elective eye surgeries and non-urgent outpatient clinics on 28 March 2020 following WHO declaration stating that COVID-19 as a Public Health Emergency Of International Concern.1 2 This was in response to the increased demands on medical services and to reduce the risk of COVID-19-related morbidity and mortality. The implementation of these measures had resulted in severe disruption to elective cataract service, which significantly prolonged waiting times. Undoubtedly, this has had a massive impact on the quality of life of our patient population.
Prior to COVID-19 pandemic, the waiting time for cataract surgery under general anaesthesia (GA) or local anaesthesia (LA) with intravenous sedation (IVS) in our ophthalmology department at Sheffield Teaching Hospitals NHS Foundation Trust was 16 weeks. In 2019, 208 patients (0.05%) and 52 patients (0.01%) out of 4587 patients underwent cataract surgery under GA and LA+IVS respectively. GA and LA+IVS waiting times have been prolonged to 36 weeks (range 30–52 weeks) due to the COVID-19 pandemic. Previously, listing patients for GA surgery or LA+IVS was less restrictive due to the availability of GA lists. In our practice, LA is usually administered by an ophthalmologist. When sedation is required alongside LA, the patient must be monitored by an anaesthetist and is operated on a GA list. Based on observation alone, a significant proportion of patients who were initially listed for cataract surgery under GA or LA+IVS eventually tolerated just LA alone. This prompted an innovative solution; suitable patients who had been on the GA and LA+IVS waiting lists for a prolonged period were counselled for LA conversion.
We describe our quality improvement project whereby ‘GA to LA conversion’ or GALA initiative was established as part of our departmental strategy to tackle our GA and LA+IVS surgical backlog.
Method
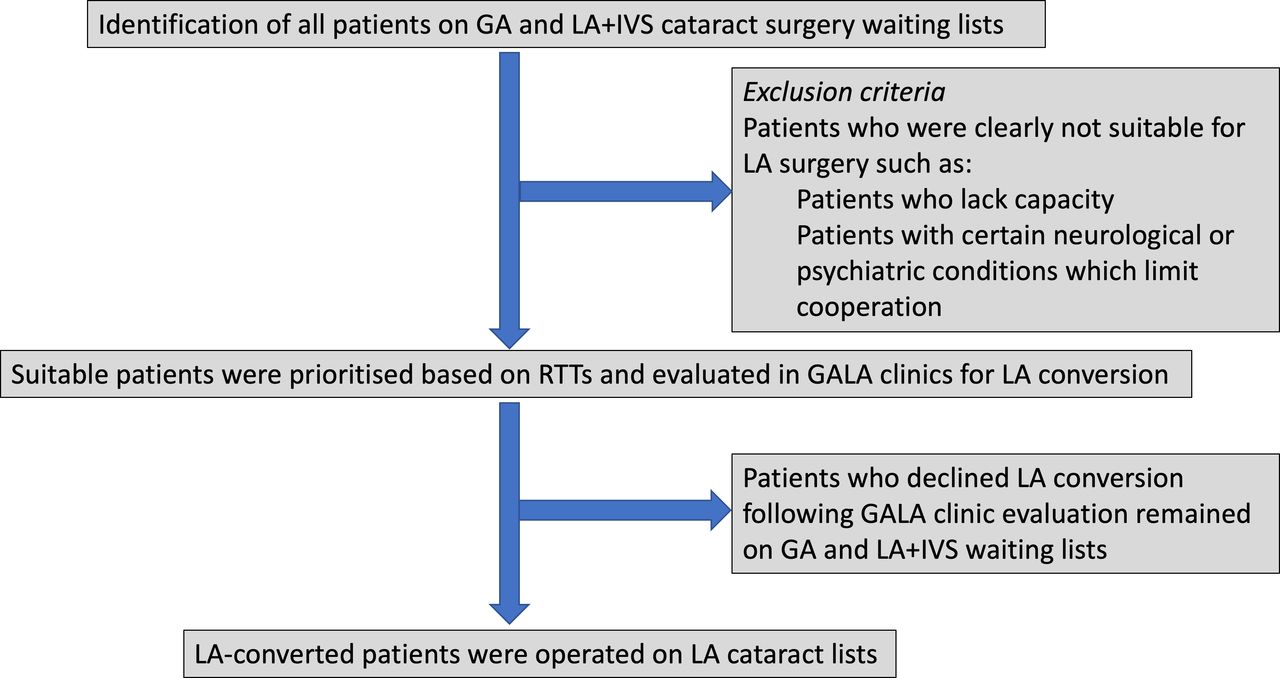
All patients on GA and LA+IVS waiting lists were identified from electronic records. Their medical histories were reviewed for LA conversion suitability. Patients who were clearly not suitable for LA, such as those with severe dementia or learning difficulties, were not included in this pilot. Suitable patients were prioritised based on their referral-to-treatment (RTT) times. Following this, patients were invited to monthly-run GALA clinic where a named surgeon (JHYT) assessed and counselled the patients for LA conversion. A personalised approach to the barriers of LA cataract surgery was offered. For example, a trial of lying on the operating table for those with severe breathlessness. A family member escort for hand holding was offered to those with panic attack. LA-converted patients were then listed for the next available LA cataract surgery lists where they underwent routine cataract surgery. Patients who declined LA conversion following GALA assessment remained on GA and LA+IVS waiting lists. The flowchart of GALA initiative is illustrated on figure 1.

{kind=link}
GALA initiative flow chart describing key steps in the process. GA, general anaesthesia; GALA, general anaesthetic to local anaesthetic conversion initiative; LA, local anaesthesia; IVS, intravenous sedation; RTT, referral-to-treatment.
Results
In this pilot scheme, 21 patients were seen in GALA clinics over a period of four months from August 2021 to November 2021. Following clinical assessment and counselling, 71% of our cohort consented for LA cataract surgery. Most of our patients had multiple ocular and systemic comorbidities which may pose as barriers to LA surgery (table 1). Our cohort consisted of patients with variable surgical complexity. Perioperative findings of the cohort included dense cataract (n=5, 36%), shallow anterior chamber (n=3, 21%), moderate dilation (n=3, 21%), deep set eyes (n=3, 21%), corneal opacity (n=1, 7%), floppy iris (n=2, 14%) and weak zonules (n=1, 7%).
Ocular and relevant systemic comorbidities of our patient cohort
Overall, 14 eyes of 13 patients were successfully operated under LA alone (Subtenon’s (n=5, 36%) and intracameral (n=9, 64%)). On the day of surgery, one case was abandoned as patient was unable to tolerate the surgical drape due to severe claustrophobia. The average age of patients included was 71 (range 31–91). Nine patients (64%) had their first eyes operated on. In five cases (36%), the draping technique had to be modified to lift drapes off the patients’ faces. In one case (7%), a family member escort had to be present in operating room. Nine cases (64%) were performed by consultant grade surgeons. The rest (36%) were performed by specialty and associate specialist (SAS) doctors (n=2) and specialty trainees (n=3). One patient (7%) had corneal oedema, which was successfully managed conservatively. All patients in this series reported subjectively better vision following LA cataract surgery. More importantly, all of them were satisfied with their experience and would consider having their second eyes done in the same way.
Overall, this patient cohort’s waiting time for cataract surgery was reduced by an average of 11 weeks. The average interval between GALA assessment clinic and LA surgery was only four weeks (range 1–16 weeks). As the GA cataract list is usually populated with four patients, the GALA initiative freed up three to four GA lists over the four months when the pilot study was run.
Discussion
The COVID-19 pandemic has demonstrated that NHS is very adaptable especially in challenging times. By converting suitable patients from GA or LA+IVS to LA listing, GALA initiative reduced cataract surgery waiting time and increased the GA list capacity for cases that genuinely require GA and sedation.
Patients with ocular comorbidities and significant perioperative findings were operated successfully under this pilot scheme. Good surgical planning was paramount; additional steps were taken perioperatively when necessary to ensure safe surgery. These included but were not limited to preoperative intravenous mannitol, preoperative intravenous methylprednisolone, usage of intracameral epinephrine, vision blue and corneal suture.
Non-consultant grade doctors were not excluded from performing cataract surgery under this pilot scheme. This shows that conversion to LA surgery does not reduce training opportunities. The resumption of training is crucial as the pandemic has led to substantial reduction in training opportunities due to redeployment, significant reductions in outpatient and surgical patient volumes.3 Careful selection of converted cases for training must be done prior to the surgery to ensure trainees’ competence in dealing with potentially more complex cases.
According to the joint statement released by RCOphth and United Kingdom & Ireland Society of Cataract & Refractive Surgeons (UKISCRS), phacoemulsification is unlikely to pose a risk of COVID-19 due to minimal viral load. All UK units are not required to treat phacoemulsification as an aerosol generating procedure (AGP). It is recommended that cataract surgery is performed under LA where possible as GA is an AGP.4 GA in elderly population is associated with exaggerated adverse effects including postoperative cognitive dysfunction.5 Conversion to LA mitigates the risks of GA, intraoperative aerosol generation and risk of COVID-19-related morbidity and mortality, especially in high risk population such as our patient cohort.6 We acknowledge that not all patients are suitable for LA conversion. Some patients with neurological or psychiatric disorders and those who lack capacity may not be cooperative during LA surgery therefore GA or LA+IVS would be more suitable.
There is a global shortage of anaesthesia workforce.7 In the UK alone, a shortage of 1400 NHS anaesthetists may delay one million surgical procedures every year.8 Conversion of GA or LA+IVS to LA listing may help with issues related to shortage of anaesthetists as they are not required to be present in theatre when patients require LA alone without sedation.
In the near future, this scheme will be expanded to include more surgeons. Following the recommendation of RCOphth and UKISCRS, patient prioritisation for the GALA initiative will be based on clinical requirements and patient factors rather than RTT alone.9 Supporting resumption of surgical training, we plan to include more trainees to perform suitable LA-converted cases in order to increase their exposures to cataract surgery.
Conclusion
In conclusion, the GALA initiative has been shown to be a safe, effective and purposeful way to reduce the waiting time of cataract surgery and to increase GA list capacity. With proper counselling, careful surgical planning, and a personalised approach to LA cataract surgery, we found that successful conversion from GA or LA+IVS to LA listing was feasible in suitable cases with good patient outcomes. By navigating through this ‘new normal era’ together and through new sustainable initiatives such as GALA, we can speed up ophthalmology service recovery, increase capacity and efficiency.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but not applicable as this is a quality improvement project exempted this study. Participants gave informed consent to participate in the study before taking part.
Footnotes
Contributors CAP was responsible for extracting and analysing data, interpreting results, creating tables and writing the manuscript. JHYT oversaw design of concept, data collection, provided feedback and final approval of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.