Article Text

Abstract
Introduction Despite a clear association between cognitive impairment and physical frailty and poor postoperative outcomes in older adults, preoperative rates are rarely assessed. We sought to implement a preoperative cognitive impairment and frailty screening programme to meet the unique needs of our rural academic centre.
Methods Through stakeholder interviews, we identified five primary drivers underlying screening implementation: staff education, technology infrastructure, workload impact, screening value and patient–provider communication. Based on these findings, we implemented cognitive dysfunction (AD8, Mini-Cog) and frailty (Clinical Frailty Scale) screening in our preoperative care clinic and select surgical clinics.
Results In the preoperative care clinic, many of our patients scored positive for clinical frailty (428 of 1231, 35%) and for cognitive impairment (264 of 1781, 14.8%). In our surgical clinics, 27% (35 of 131) and 9% (12 of 131) scored positive for clinical frailty and cognitive impairment, respectively. Compliance to screening improved from 48% to 86% 1 year later.
Conclusion We qualitatively analysed stakeholder feedback to drive the successful implementation of a preoperative cognitive impairment and frailty screening programme in our rural tertiary care centre. Preliminary data suggest that a clinically significant proportion of older adults screen positive for preoperative cognitive impairment and frailty and would benefit from tailored inpatient care.
- Anaesthesia
- Surgery
- Quality improvement
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Cognitive impairment and physical frailty are associated with poor postoperative outcomes in older adults and are rarely assessed preoperatively.
What this study adds?
Preoperative cognitive impairment and frailty screening can be successfully implemented by a multidisciplinary team in the preoperative setting. In our rural institution, a clinically significant portion of older adults screened positive for preoperative cognitive impairment and physical frailty.
How this study might affect research, practice or policy?
Patients who screen positive for preoperative cognitive impairment and frailty may benefit from tailored inpatient care. Multidisciplinary efforts dedicated to the postoperative care of older adults may improve outcomes in this vulnerable patient population.
Introduction
Currently adults age 65 and older account for greater than 40% of all inpatient surgeries and, according to recent studies, 10%–25% of these patients have preexisting cognitive impairment.1 2 Preoperative cognitive impairment and physical frailty increase a patient’s risk of developing postoperative complications including increased length of stay, readmission, delirium and higher morbidity and mortality.3–9 Further, it has been shown that patients with postoperative cognitive dysfunction experience a two times greater impairment in activities of daily living than those without.10
Older surgical patients are a heterogeneous group, including many who continue to work and exercise vigorously, but also those who are limited by medical and cognitive issues. Hence, there is a need to perform preoperative screening to risk stratify and support patients with impairment. The recently instituted American College of Surgeons (ACS) Geriatric Surgery Verification Programme establishes surgical standards for the care of older surgical patients, and includes comprehensive preoperative vulnerability screening.1 The ACS, American Geriatrics Society and American Society of Anesthesiology Brain Health Initiative have all promoted preoperative cognitive and frailty screening for almost a decade with variable adherence.1 11 12 A recent study found that the uptake of screening has been poor (<30%) among anaesthesiologists, often seen as leaders in preoperative testing, and cited lack of time and knowledge of how to operationalise a screening programme as barriers to implementation.12
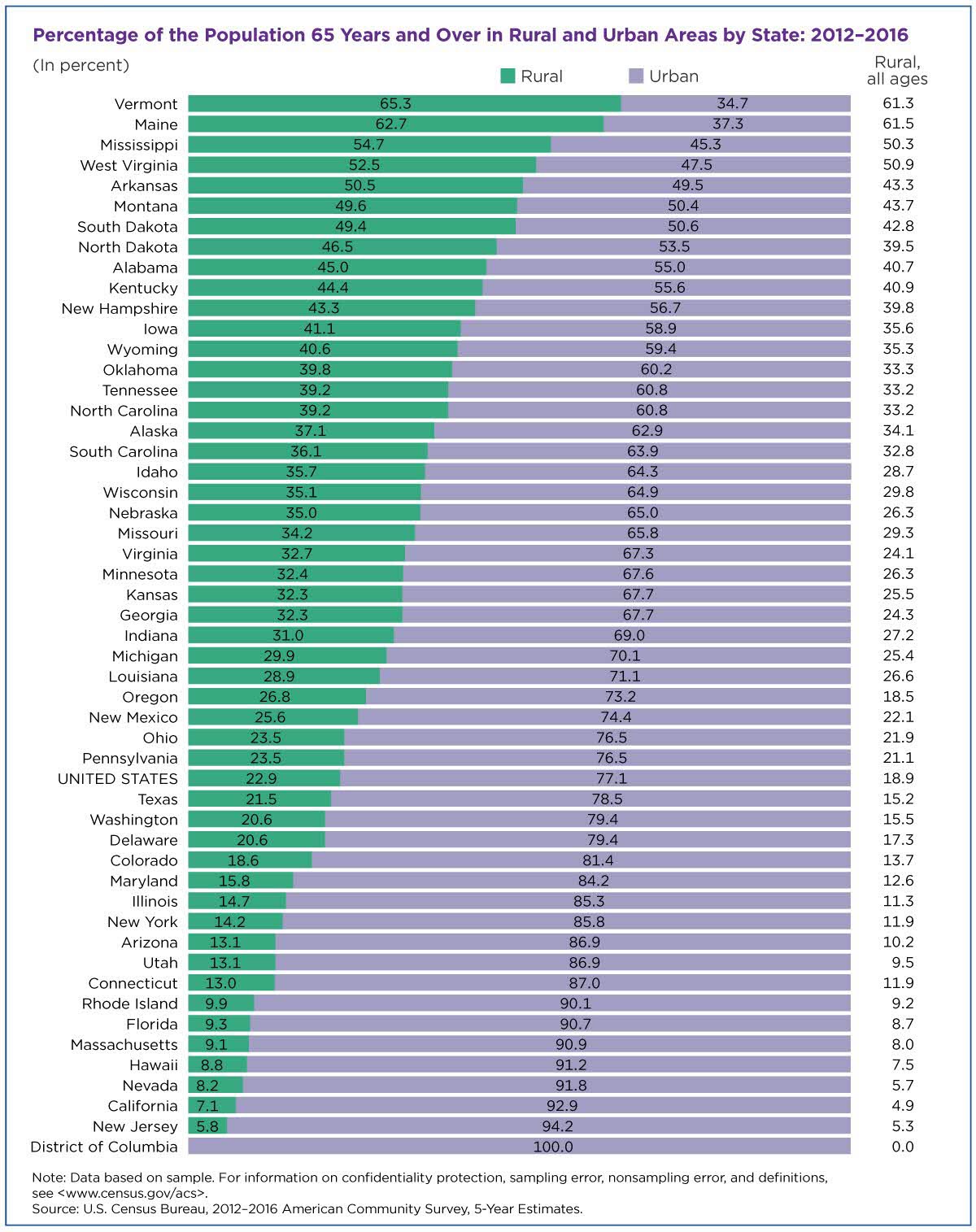
Dartmouth Hitchcock Medical Center (DHMC) is an academic, tertiary medical centre with a catchment area that includes the states of New Hampshire and Vermont. The population in New Hampshire and Vermont are among the oldest in the USA, with approximately 18.7% of New Hampshire’s population and 20.0% of Vermont’s reported as older than 65 years.13 Further, 40% of this geriatric population in New Hampshire and 65% in Vermont live in rural areas.14 15 Older surgical patients in rural areas face additional challenges. One-quarter of adults over 65 live in rural areas, but only ten percent of geriatric trained healthcare specialists work in non-urban centres.16–18 Access to primary care in rural New England is especially limited, with Medicare eligible patients spending approximately 33% fewer days with their primary providers than patients in urban settings.19 Due to the limited access to rural primary care and geriatric-trained providers, we recognise the need for cognitive impairment and frailty screening to be performed by anesthesiology and surgery in the preoperative setting.
We sought to implement preoperative cognitive impairment and frailty screening for older surgical patients in our rural academic medical centre. Our intention was to design a screening programme that did not rely on additional specialist involvement and could be further implemented in resource constrained community hospitals.
Methods
Clinical setting
DHMC is a 396-bed tertiary care centre located in rural New Hampshire. It is the only academic centre and level-1 trauma centre in the state of New Hampshire and is certified as an Institute for Healthcare Improvement Age-Friendly Health Centre. More than 10 000 patients over age 65 present for surgery at DHMC every year, representing approximately 37% of our total surgical volume. Our programme specifically focuses on the subset of older adults who present for elective surgical procedures with a planned postoperative hospitalisation, accounting for approximately 2600 procedures annually.
Intervention and implementation design
We assembled a multidisciplinary team—including Surgery, Anesthesiology, Geriatrics, Nursing, Case Management, Dementia Resource Specialists and members of our Ageing Resource Centre—to provide early input regarding the patient experience so that an effective screening process centered on patient needs could be designed. After formation of our multidisciplinary team, we conducted stakeholder interviews with older surgical patients, nurses, medical assistants and surgeons, to assess the perceptions of cognitive impairment screening as well as the concerns and needs of providers along the perioperative workflow.
Through stakeholder interviews, we identified five primary drivers underlying successful screening implementation: staff education, technology infrastructure, workload impact, screening value and patient–provider communication. To address workload impact and screening value, we introduced short, validated tools that took 5 minutes or less to complete. Nurses and medical assistants received education on the screening flowsheets (AD8 Dementia Screening, Mini-Cog, and Clinical Frailty Scale, CFS) as well as information on who to screen, how to screen, and how to normalise the screening and alleviate patient concerns about the results. Screening education included an initial training session followed by biweekly visits to address any questions and/or concerns regarding the screening process. We used our biweekly visits to share data on screening compliance as well as the rate of positive cognitive impairment and frailty screens among our older surgical patients. During these sessions, we used material aids to assist with education. Nurses and medical assistants expressed a desire to understand the downstream effects of screening, so we provided further teaching on our programme’s global implications including but not limited to postoperative delirium screening. Furthermore, our end-users agreed on the need to use a technologic foundation to improve screening adherence. We worked with our information technology personnel to embed screening flowsheets into our electronic health record (EHR) and provide in-depth instruction regarding the screening tool. Positive screens are followed by automatic EHR best practice advisories to guide future management (see figure 1).

Electronic Medical Record Best Practice Advisories for Postoperative Delirium Prevention. *The Dartmouth Health Information Technology Department designed the electronic health record best practice alerts (pictured above). ‘Snowy owl is a named used in electronic health practice environments and is not a real person.
Patient–provider communication was an additional driver that had interesting findings from both our patient and provider stakeholder interviews. We encountered a reluctance expressed by older adults regarding the use of cognitive impairment and frailty screening. Patients feared the label, ‘cognitive impairment’ and the implication it might have on future healthcare encounters. We discovered that replacing the term ‘cognitive impairment screening’ with ‘brain health screening’ improved patients’ perception of the screen. Those performing the screening emphasised that the screen was not a test, but rather a measurement like blood pressure.
Initial screening roll-out began in our anesthesiologist-led perioperative care clinic (PCC) for adults aged 65 and older. The AD8 screening for cognitive impairment was chosen because it is a well-validated, short cognitive assessment that can be administered over the phone, which was essential given the early phases of our programme coincided with the COVID-19 pandemic. Additionally, many of our patients do not physically attend clinic due to transportation issues or long travel distances making the virtual nature of the AD8 tool especially useful. The AD8 screening tool was undergoing its pilot phase prior to our programme implementation in February 2021, but we aimed to improve screening adherence through additional supportive resources, including staff education and stakeholder involvement. Thus, nurses received specific training and feedback on practice patterns from a physician and a medical assistant dyad who were experienced in the assessments of patients with dementia. We introduced the CFS screening in our PCC in February 2021 and used the same techniques as listed above to ensure nurses were adequately trained and comfortable with the assessment.
We collaborated with our EHR support team to embed our screening protocol into the preoperative workflow for nurses and anaesthesia providers, prompting the user to perform the assessment only for patients aged 65 and older, while also automatically scoring and recording the result. A positive screen automatically generates a ‘banner’ in the patient’s chart to alert all providers of the patient’s increased risk for delirium and triggers a set of perioperative best-practice advisories for delirium prevention for the anaesthesia team (see figure 1).
Since only 40% of our older surgical patients attend the PCC, we realised that screening would need to be implemented in surgical clinics at the time of consultation to evaluate a larger proportion of the geriatric surgical population. We piloted our screening programme in three clinic areas with surgeon champions: neurosurgery, general surgery and urogynecology. In our surgical clinics, we implemented Mini-Cog screening for cognitive dysfunction due to its low interobserver variability as well as its validation in geriatric surgical patients. The Mini-Cog is a simple, validated and brief cognitive screening tool that assesses impairment through a three-item memory recall and a clock drawing component. In our surgical clinics, a positive Mini-Cog and/or CFS triggers an EHR-based prompt for surgeons to refer patients to our Ageing Resource Centre, where a thorough chart review is performed and social determinants of health intake as well as case management queries are reviewed. If needed, the patient may be referred to a Geriatrician for further assessment and presurgical medical optimisation.
Results
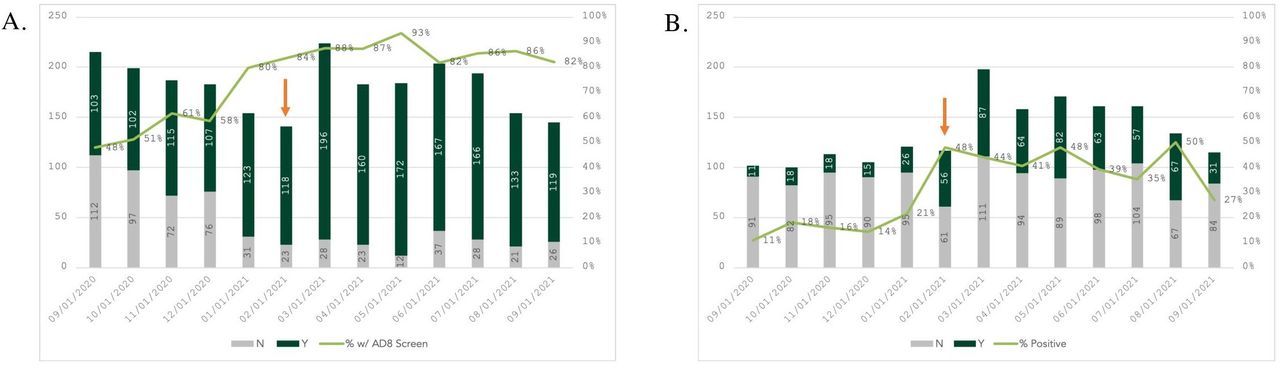
Between September 2020 and January 2021, 59% (550 of 938) of eligible patients were screened for cognitive impairment in our PCC. With programme implementation, 86% (1231 of 1429) of eligible patients were screened for cognitive impairment between February 2021 and September 2021 (see figure 2). Over a 1-year period, 14.8% (264 of 1781) of older adults who underwent screening screened positive for cognitive dysfunction in the PCC. Clinical frailty screening was implemented in the PCC starting in February 2021 and between February 2021 and September 2021, 35% (428 of 1231) of older adults who underwent screening screened positive for clinical frailty.
{kind=link}
{kind=link}
A. AD8 Cognitive Impairment Screening Adherance in the Preoperative Care Clinic B. Prevalence of Positive Cognitive Impairment and/or Fraility Screening in the Preoperative Care Clinic. *Red arrow indicates the first month of our QI program initiative. Clinical Frailty Screening also introduced at this time in our Preoperative Care Clinic.
Surgical clinic preoperative cognitive impairment and frailty screening began in July 2021 (see online supplemental figure 1). Between July 2021 and October 2021, 27% (35 of 131) of older adult patients who underwent screening screened positive for clinical frailty, while 9% (12 of 131) screened positive for cognitive dysfunction. In our surgical clinics, six patients who screened positive for cognitive dysfunction, frailty or both have been referred to our Ageing Resource Centre for further preoperative evaluation.
Supplemental material
Discussion
Our screening protocol used a multidisciplinary approach to implement preoperative cognitive impairment and frailty screening at a rural academic centre. Through stakeholder interviews, we tailored the screening programme to the needs of patients and staff at our institution. Supportive measures to ensure implementation included frequent staff education, EHR enhancements, minimization of time demands, feedback on the value and impact of screening and patient–provider communication. Through these efforts, we increased adherence to AD8 cognitive impairment screening in our PCC from 48% to 86% over a 1-year period.
Our quality improvement report demonstrates that positive preoperative cognitive impairment and/or frailty screening is significant in our rural institution. In our PCC, 35% of eligible patients screened positive for clinical frailty while 14.8% screened positive for cognitive impairment. In our surgical clinics, 27% of eligible older adult patients screening screened positive for clinical frailty, while 9% screened positive for cognitive dysfunction. The proportion of clinical frailty and cognitive impairment is in-line with published data for the age group, with most reporting a broad range of preoperative cognitive dysfunction and clinical frailty between 15%–63% and 10%–65% of patients, respectively.20 21 The variation in positive cognitive impairment screens between the PCC and surgical clinics (14.8% vs 9%) may represent distinctions between the screening tools we used (AD8 vs Mini-Cog). In a recent meta-analysis, the AD8 tool used was found to have a higher sensitivity (0.72) than specificity (0.67), making false positives more likely.22 In comparison, the Mini-Cog screening tool has been reported to have a higher sensitivity of 0.91 and specificity of 0.86.23 However, we used the same frailty screening tool in our PCC and surgical clinics with a similar variation in positive clinical frailty screens (35% vs 27%) indicating that there may be notable differences between the patient populations seen in the various screening environments.
To implement a successful and sustainable screening programme we used a hybrid implementation-effectiveness design. This healthcare redesign process placed an equal emphasis on clinical implementation and effectiveness, which allowed us to tailor our programme to the needs of our end-users before waiting for effectiveness data. Previous work by Donovan et al used a similar hybrid design to implement a perioperative delirium prevention pathway.24 This programme was set in an urban healthcare setting with a wider array of resources available, including a hospital-wide Delirium Reduction Campaign. However, using comparable techniques including stakeholder involvement, continual feedback and EHR enhancements, the authors were able to significantly reduce administration of Beers Potentially Inappropriate Medications in the perioperative setting.24 Of note, the American Geriatric Society Beers Criteria is an explicit list of medications that should typically be avoided in older adults.25 Our programme design encountered similar success as evidenced by the increase in AD8 cognitive impairment screening adherence in our PCC from 46% to 86% with programme implementation.
Our findings have several limitations with respect to external generalisability. Our programme was specifically designed to meet the needs of our rural academic institution and may require modifications for centres that are more urban or not academic based. Our EHR enhancements were tailored to our home medical record and may not easily translate to healthcare settings with different EHR systems or paper-based medical records. We do not yet know whether our screening programme will translate into better clinical or patient centred outcomes in our population. In future studies, we aim to correlate positive cognitive impairment and frailty screening with adherence to perioperative delirium prevention best practices as well as postoperative delirium incidence. We are also building the infrastructure for a delirium prevention volunteer service, which will assist with patient reorientation, maintaining day-night cycles and ensuring access to assistive devices. Furthermore, we aim to expand our geriatric specific EHR enhancements to our entire referral area with potential to improve geriatric surgical care to the most rural community healthcare facilities in New Hampshire. Further research is needed to assess if our interdisciplinary geriatric-specific workflow can decrease postoperative delirium rates, improve patient satisfaction scores and decrease overall healthcare spending through decreased length of stay.
Conclusions
We developed a multidisciplinary perioperative programme focused on preoperative identification of cognitive impairment and frailty. Through qualitative evaluation of stakeholder needs we created a workflow for preoperative cognitive and frailty screening that was customised to the needs of our rural institution. During our pilot period, we identified a clinically significant portion of older adult surgical patients who screened positive for preoperative cognitive impairment and frailty. Additionally, we were able to increase screening adherence through stakeholder engagement and feedback. Going forward, we will correlate programme uptake with postoperative delirium incidence, length of stay and patient satisfaction scores. This screening programme is a key step in improving perioperative geriatric care by providing a reliable mechanism to identify and target the patients who need our close attention and care the most.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank the DH CARES team for their continued efforts with implementation of preoperative cognitive impairment and frailty screening.
References
{kind=link}
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CDA: conceptualisation, literature review, writing original draft, review and editing, figures, data interpretation. CF: review and editing, figures, data interpretation, data analysis, stakeholder interviews. KC: data collection, data analysis, data interpretation, review and editing, figures. DG: review and editing, protocol implementation. VC: review and editing, supervision. AA: review and editing, supervision. AB: review and editing, supervision, stakeholder interviews. SD: supervision, review and editing, conceptualisation, guarantor.
Funding This work was supported by the Susan & Richard Levy Health Care Delivery Incubator, a joint venture between The Dartmouth Institute for Health Policy & Clinical Practice (TDI) and Dartmouth-Hitchcock Health (D-HH).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.