Article Text

Abstract
Introduction Sepsis is a common cause of emergency department (ED) presentation and hospital admission, accounting for a disproportionate number of deaths each year relative to its incidence. Sepsis outcomes have improved with increased recognition and treatment standards promoted by the Surviving Sepsis Campaign. Due to delay in recognition and other barriers, sepsis bundle compliance remains low nationally. We hypothesised that a targeted education intervention regarding use of an electronic health record (EHR) tool for identification and management of sepsis would lead to increased EHR tool utilisation and increased sepsis bundle compliance.
Methods We created a multidisciplinary quality improvement team to provide training and feedback on EHR tool utilisation within our ED. A prospective evaluation of the rate of EHR tool utilisation was monitored from June through December 2020. Simultaneously, we conducted two retrospective cohort studies comparing overall sepsis bundle compliance for patients when EHR tool was used versus not used. The first cohort was all patients with intention-to-treat for any sepsis severity. The second cohort of patients included adult patients with time of recognition of sepsis in the ED admitted with a diagnosis of severe sepsis or septic shock.
Results EHR tool utilisation increased from 23.3% baseline prior to intervention to 87.2% during the study. In the intention-to-treat cohort, there was a statistically significant difference in compliance between EHR tool utilisation versus no utilisation in overall bundle compliance (p<0.001) and for several individual components: initial lactate (p=0.009), repeat lactate (p=0.001), timely antibiotics (p=0.031), blood cultures before antibiotics (p=0.001), initial fluid bolus (p<0.001) and fluid reassessment (p<0.001). In the severe sepsis and septic shock cohort, EHR tool use increased from 71.2% pre-intervention to 85.0% post-intervention (p=0.008).
Conclusion With training, feedback and EHR optimisation, an EHR tool can be successfully integrated into current workflows and appears to increase sepsis bundle compliance.
- quality improvement
- critical care
- emergency department
- standards of care
- decision support
- computerised
Data availability statement
No data are available. No data from this study are available for reuse by other work groups.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Sepsis is a syndrome characterised by life-threatening organ dysfunction resulting from a dysregulated host response to infection.1 Presence of organ dysfunction (previously termed ‘severe sepsis’)2—identified by an increase in Sequential (sepsis-related) Organ Failure Assessment score of two or more points—is associated with an in-hospital mortality rate of greater than 10%. Septic shock—defined as a vasopressor requirement to maintain a mean arterial pressure of 65 mm Hg or greater and/or serum lactate level greater than 4 mmol/L in the absence of hypovolemia—is characterised by profound circulatory, cellular and metabolic abnormalities and is associated with in-hospital mortality rates of greater than 40%.1
At least 1.7 million adults in the USA develop sepsis each year,3 4 with a majority of patients with sepsis presenting through the emergency department (ED).5 6 Nearly three-quarters of ED patients with sepsis are admitted to the hospital, with one-quarter requiring admission to the intensive care unit.5 While comprising only 6% of hospital admissions,3 sepsis accounts for one-third of in-hospital mortality.4
Prior to 2001, no standard existed for early treatment of sepsis and septic shock, and the sepsis mortality rate was 40%–50%.7 Early goal-directed therapy marked the beginning of bundled sepsis care and began an era of significant improvement in sepsis mortality.8 Further advances in sepsis resuscitation and research over the next two decades9–11 led to the development of the Society of Critical Care Medicine Surviving Sepsis Campaign (SSC) guidelines for early identification and treatment of patients with sepsis.12 The SSC guidelines, which outline bundled care elements that must be completed within hours of sepsis recognition, have been associated with improved outcomes, including reduced mortality.13 14 The Centers for Medicare and Medicaid Services (CMS) has subsequently developed the Severe Sepsis/Septic Shock Early Management Bundle (SEP-1), which impacts hospital reimbursement for care of patients with sepsis, signifying a new standard of care. Several Departments of Health, including New York State, have adopted similar management bundles.
Despite these advances, significant barriers to total bundle compliance exist due to patient, staffing, ED environment and training factors.15 Overall bundle compliance for hospitals contributing to the SCC database is reported as 21.5%,13 and for the New York State bundle, compliance was 36.1% in the most recently published data.16 As a response, departmental quality improvement projects are common. In one study of 50 EDs, 92% of sites reported participating in at least one project regarding sepsis bundle care,17 indicating a strong desire for improvement.
Nationally, more than 50% of patients admitted for sepsis through the ED experience boarding times of greater than 4 hours,5 signifying the pivotal role the ED holds in providing sepsis care. Several studies describe different EDs’ experience in quality improvement projects aimed at improving sepsis bundle compliance and care. Prior interventions have included electronic health record (EHR) driven ‘sepsis alerts’18–24; EHR or printed physician order sets18 21 23–28; printed algorithms or protocols for physicians22 25; nursing narrators or protocols18 29 30; sepsis huddles and improved screening23 28 31; and training, education, feedback or other continued communication.24 25 32 Collectively, these improvement processes are associated with increased timely administration of appropriate antibiotics,18–20 22 27 29 30 increased timely administration of intravenous fluids,18 22 increased appropriate measurement of serum lactate,29 30 increased collection of blood cultures before antibiotics,29 increased overall sepsis bundle compliance,18 21 28 29 31 32 decreased sepsis-related rapid response teams from inpatient units,31 decreased need for vasopressors,27 decreased need for mechanical ventilation,23 24 decreased hospital length of stay,23 24 29 decreased intensive care unit length of stay23 24 and decreased in-hospital mortality.21 23 24 27 31
Our hospital sees a substantial volume of patients with sepsis, with more than 650 inpatient admissions with severe sepsis and septic shock annually. The ED accounts for over 65% of all cases at the time of recognition. Throughout years 2015–2019, there was an initiative focused on sepsis care leading to an increase in 6-hour bundle compliance from 40% to nearly 80%. During the height of the COVID-19 pandemic, there was an institutional concern for a decrease in sepsis bundle compliance, as was the trend nationally. Furthermore, an EHR tool—including a sepsis alert, provider order set (‘navigator’), and nursing sepsis ‘narrator’—was disseminated in our ED in September 2019 and was noted to be underused since its launch (online supplemental files 1–3). For these reasons, in May 2020, we developed a multidisciplinary quality improvement initiative focused on training on the use of the EHR tool, re-education of sepsis bundled care, targeted feedback and EHR tool improvement.
Supplemental material
Supplemental material
Supplemental material
The purpose of this study is to evaluate whether our interventions led to increased EHR tool usage and if EHR tool usage was associated with higher sepsis bundle compliance. We hypothesised that EHR tool usage would increase after our quality improvement intervention and that EHR tool usage would correlate with higher SEP-1 sepsis bundle compliance.
Methods
Setting
NYU Langone Hospital—Brooklyn is a 450 bed, academic hospital setting with nearly 14 000 inpatient admissions and approximately 80 000 ED visits annually. The hospital ranks in the top tier for sepsis care in New York State according to New York State Department of Health Reporting Registry.
The multidisciplinary team initially met in May 2020 in which the scope of work and project charter development took place. The objective of this effort was to promote appropriate use of the sepsis EHR tool and monitor bundle compliance over time as it relates to EHR tool usage.
Population
A retrospective cohort analysis was completed for all adult (18 years and older) ED patients who were treated as possible sepsis in the ED from 1 May 2020 through 31 December 2020. Adult patients with sepsis care activated in the ED, either secondary to a lactate >2 mmol/L, presence of two or more systemic inflammatory response syndrome (SIRS) criteria with suspicion for bacterial infection, and/or provider-initiated care for other reasons (suspected bacterial source of infection and other markers of organ dysfunction, and so on) were included. This cohort included patients identified in the ED with an intention-to-treat as sepsis and included patients with sepsis, severe sepsis and septic shock as well as patients with suspected sepsis who ultimately had an alternate diagnosis.
For further retrospective review over time, all adult (18 years and older) patients who were admitted and coded by discharge International Statistical Classification of Diseases and Related Health Problems 10th Edition (ICD-10) codes as severe sepsis or septic shock with time of recognition in the ED were evaluated for overall SEP-1 3-hour and 6-hour bundle compliance, individual metric compliance and mortality as a secondary outcome. This second cohort represents all patients with sepsis who had data submitted to CMS from 1 September 2019 through 31 December 2020. The New York State sepsis care reimbursement structure is based on hospital discharge diagnosis codes (ie, ICD-10),33 which use the sepsis-2 definitions of severe sepsis and septic shock.2
Medical chart review and data acquisition was performed as part of a quality improvement analysis and, as such, was exempt from institutional review board approval.
Design
Intervention
The framework for the process improvement was based on the Lewin’s three-step change management model.34 The model consists of three steps in order to implement change: unfreezing (changing human behaviour or mindset); changing (implementing change driven by education and leadership influence) and refreezing (promoting and sustaining the change into practice). The multidisciplinary team (sepsis work group) included physician and nursing leadership, nurses, attending and resident physicians, physician assistants (PAs), administrative assistants, computer support, quality analysts, pharmacists and inpatient medicine physicians.
A multi-pronged intervention included the following: (1) nurse focused education and reiteration of EHR sepsis narrator tool launch and usage for sepsis recognition and management; (2) nurse, physician and PA directed education on bundle components and interaction with the provider navigator; (3) nurse, physician and PA group and individualised feedback related to the use of the EHR tool for improved utility and effectiveness in addition to bundle components and compliance. Educational components included in-person direct training, email and verbal communication, and case-specific provider-directed feedback for any non-adherence. To further prepare staff for the implementation of this initiative, multifaceted education was provided to all care teams electronically and in person, and sepsis care reminders were posted on all ED computer screens prior to the ‘Go-Live’ of the project. In this pre-implementation phase, education was focused on recognition of sepsis and process for EHR tool utilisation. Recognition teaching for providers (attendings, residents and PAs) focused on the differentiation of sepsis, severe sepsis and septic shock. Providers were educated on sepsis laboratory criteria for end organ damage. Nursing efforts were focused on recognition of SIRS. Process education for providers included education on components of bundle care and use of the EHR navigator, which contains all appropriate orders to meet sepsis bundle compliance. Process education for nursing included prompting of initiating a sepsis huddle when SIRS criteria were met and description of how to properly document when using the EHR sepsis narrator and complete the components of bundle care. The implementation phase, starting 1 June 2020, is ongoing, focuses on continued outcome education through direct feedback from the sepsis work group on missed cases and misuse of EHR tool as well as positive feedback when excellent bundle care is achieved (online supplemental file 4).
Supplemental material
During the initial phase of project planning, on-site informal feedback was elicited from providers and nurses to help identify barriers to sepsis bundled care and EHR tool utilisation in the ED. The EHR narrator and navigator went through several iterations prior to implementation as a result of direct verbal and written nursing and provider feedback. Throughout the implementation phase, team members directly observed interaction with the EHR tool and elicited feedback from users to assist in making changes to the EHR tool to make it more effective and easier used. Ongoing feedback continues to be obtained by the sepsis work group to optimise usability and utilisation of the EHR sepsis tool. The initial educational intervention did not undergo direct evaluation from trainees.
Once a patient is identified as possible sepsis, either by lactate ≥2 mmol/L (which triggers an EHR notification (‘Best Practice Alert’ (BPA)) to the ED provider and nurse), two or more SIRS criteria with suspicion for bacterial infection (which triggers a BPA to the ED provider and nurse), or any other ED provider initiation, the primary nurse and ED provider (attending with or without resident or PA) perform a bedside huddle. The purpose of the huddle is to decide if the patient has sepsis and should be initiated on the sepsis bundle care protocol or not, which is at the primary physician’s discretion. Once it is decided that a patient is starting on the sepsis protocol, the EHR tool is then launched. Sepsis bundle care and corresponding checklist items are carried out with prompts and reminders specific to the provider and nurses sent through the EHR. When all care is complete, the sepsis EHR tool can be marked complete. The workflow for identification of patients with sepsis and initiation of the sepsis protocol is summarised in online supplemental file 5.
Supplemental material
Evaluation
Throughout the pre-education and implementation period from 1 May 2020 to 31 December 2020, ED patients who were treated as possible sepsis were prospectively observed to monitor usage of the EHR tool. The data obtained for this observation included the utilisation of the EHR tool as it relates to the compliance with bundle interventions. Overall monthly rates were calculated to monitor the utilisation of the EHR tool over time.
A retrospective cohort analysis was completed for all adult ED patients who were treated as possible sepsis in the ED. This cohort included patients identified in the ED with an intention-to-treat as sepsis and included patients with sepsis, severe sepsis and septic shock as well as patients with suspected sepsis who ultimately had an alternate diagnosis. Chart review for this cohort consisted of sepsis EHR tool utilisation in addition to overall bundle compliance as well as individual components of sepsis care compliance from 1 May 2020 to 31 June 2020, including:
Initial lactate.
Blood cultures before antibiotics.
Appropriate antibiotics (administration in less than 3 hours).
And when applicable:
Intravenous fluid administration.
Vasopressor administration.
Repeat lactate (for initial lactate >2 mmol/L).
Vital sign reassessment.
Differences in bundle compliance between the two groups (EHR tool used vs EHR tool not used) were analysed for significance using Pearson χ2 test at the α-level=0.05.
An additional retrospective cohort analysis was performed on all patients from 1 September 2019 to 31 December 2020, who were identified as having severe sepsis or septic shock based on inpatient discharge ICD-10 codes whose time of recognition began in the ED. The overall rates of SEP-1 3-hour and 6-hour bundle compliance were compared for patients with EHR tool used versus not used. Similarly, individual bundle components, overall bundle compliance and mortality were compared with pre-implementation and post-implementation of our quality initiative (1 September 2019 to 30 May 2020 vs 1 June 2020 through 31 December 2020). Variables were analysed for statistical significance at the α-level=0.05 using Mann-Whitney non-parametric test. All analyses were conducted using SAS V.9.4.
Patient and public involvement
The development of the research question was designed to improve quality of care provided for patients presenting to the ED with sepsis. Patients were not involved in formulating the research question, design of, recruitment to, or conduct of the study. Results of the research intend to be disseminated via open access publication.
Results
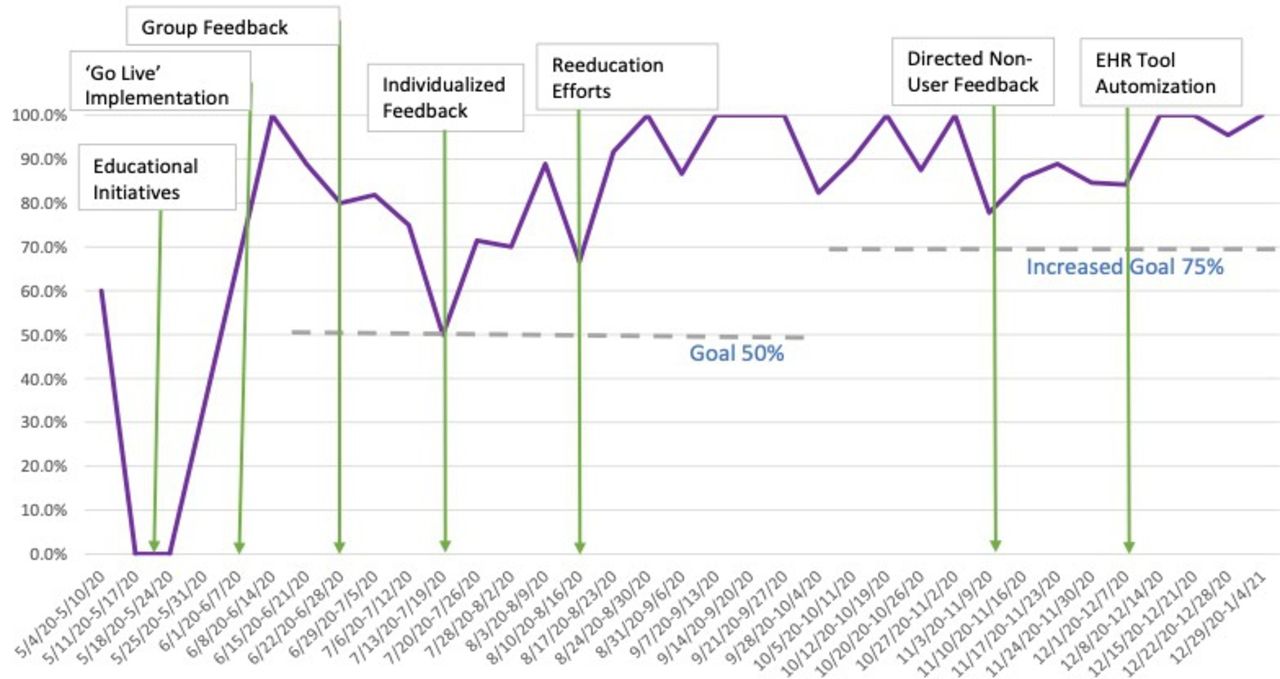
The multifaceted initiative focused on education, feedback, EHR tool optimisation and coinciding huddle and checklists for sepsis bundle adherence was initiated in May 2020 and launch for implementation started on 1 June 2020. The implementation involved 112 nurses, 66 physicians and 17 PAs across one hospital system ED. EHR tool usage and bundle compliance was recorded for a total of 373 patients over 8 months (1 May 2020 to 31 December 2020). The timing of interventions as it relates to the rates of EHR tool utilisation is illustrated in figure 1.

Quality initiative implementation and prospective EHR tool utilisation. EHR tool utilisation was analysed prospectively starting May 2020. Here, weekly percentage of patients identified as having sepsis in the ED in which the EHR tool was used over time is shown in relation to specific quality interventions. ED, emergency department; EHR, electronic health record.
Throughout the study period, the monthly rates of EHR tool utilisation for all adult patients identified as presenting with sepsis in the ED were recorded. Overall EHR tool utilisation increased by 63.9%, from 23.3% baseline prior to intervention to an average 87.2% during the implementation phase of the study.
A retrospective cohort analysis was completed for 114 adult ED patients with an intention-to-treat as sepsis based on sepsis activation for lactate ≥2 mmol/L, two or more SIRS and concern for bacterial infection, or ED provider discretion over a 2 month period, 1 month pre-implementation and 1 month during implementation. Overall 6-hour bundle compliance was compared for patients with EHR tool usage and without EHR tool usage and was 62.2% and 37.8%, respectively. There was a statistically significant difference in compliance between EHR tool utilisation versus no utilisation in overall bundle compliance (p<0.001) and for the following bundle components: initial lactate (p=0.009), repeat lactate (p=0.001), timely antibiotics (p=0.031), blood cultures before antibiotics (p=0.001), initial fluid bolus (p<0.001) and vital signs reassessment after fluids (p<0.001). These findings are summarised in figure 2.

Bundle component compliance as it relates to EHR tool utilisation. Percentage of patients with intention-to-treat as sepsis meeting each individual SEP-1 metric (initial lactate, repeat lactate when applicable, blood cultures before antibiotic administration, appropriate antibiotics, intravenous fluid bolus administration (30 cc/kg), vital sign/fluid status reassessment after fluid resuscitation, and vasopressor administration when appropriate) when the EHR tool was used (blue) versus not used (orange). ‘Bundle compliance’ is achieved if every metric is completed. EHR, electronic health record; SEP-1, Severe Sepsis/Septic Shock Early Management Bundle.
A separate retrospective cohort analysis was completed for 563 adult patients admitted from the ED and discharged with the ICD-10 code of severe sepsis or septic shock with time of recognition occurring in the ED over 16 months spanning the time prior to, during and after the implementation phase of the study.
Among all patients in the cohort, there were 75.1% patients in whom providers used the EHR tool and passed the 6-hour bundle, 20.4% of patients in whom the EHR tool was not used and failed the bundle, 3.4% of patients in whom EHR tool was not used and passed the bundle and 1.1% of patients in whom EHR tool was used and failed the bundle.
For all patients in this cohort where EHR tool was used, 98.6% passed the 6-hour bundle and 1.4% failed. For patients in whom the EHR tool was not used, 14.2% passed the 6-hour bundle while 85.8% failed. See figure 3 for the monthly distribution.

Bundle compliance as it relates to EHR tool utilisation. Percentage of patients with CMS discharge diagnoses of ‘severe sepsis’ or septic shock with time of identification in the ED grouped by EHR tool utilisation and pass (all metrics completed) or fail (one or more metrics not completed) of the sepsis bundle by time in months. CMS, Centers for Medicare and Medicaid Services; ED, emergency department; EHR, electronic health record.
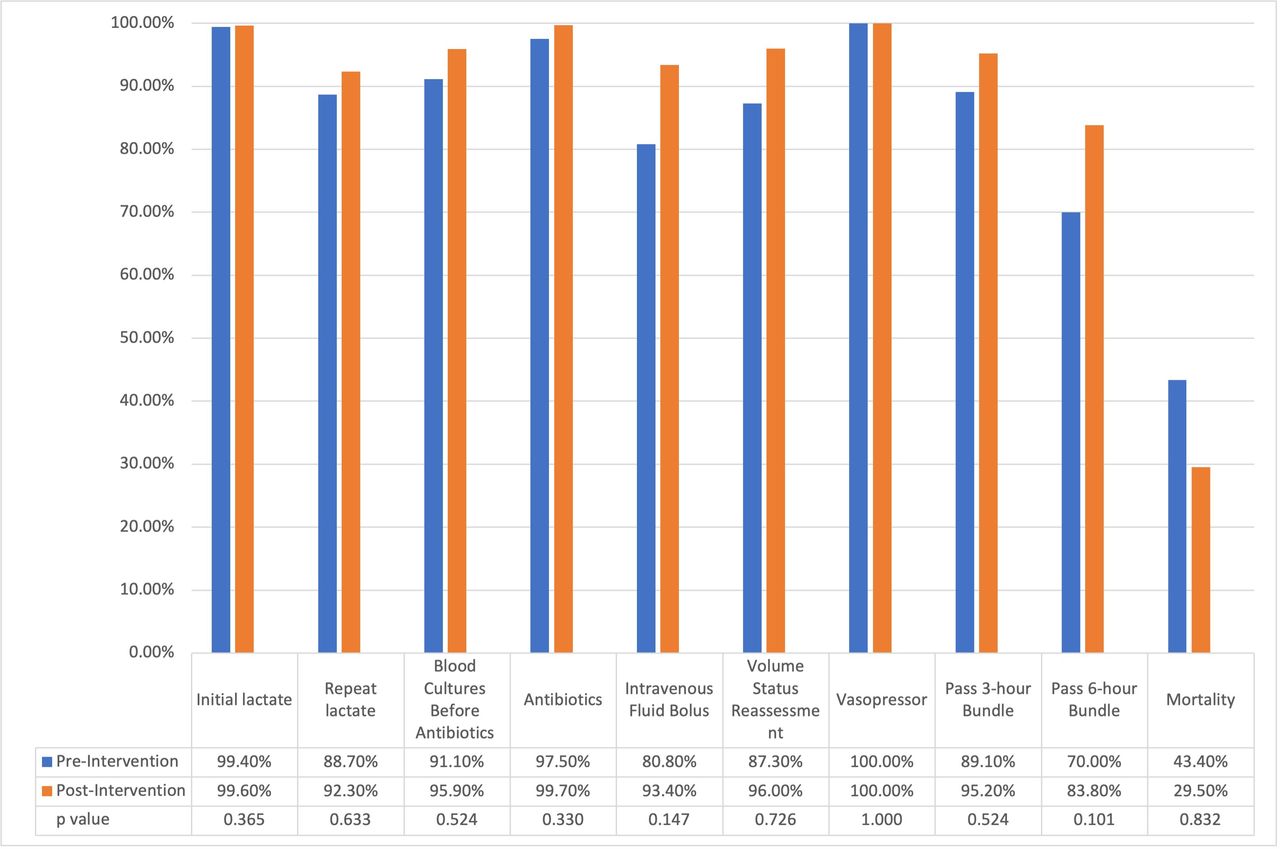
In this same population of 563 patients discharged as severe sepsis or septic shock with time of onset in the ED, sepsis bundle compliance pre-quality improvement intervention (from 1 September 2019 to 31 May 2020) and post-intervention (from 1 June 2020 to 31 December 2020) were also compared regardless of EHR tool utilisation. In this retrospective cohort study, EHR tool utilisation increased from 71.2% pre-intervention to 85.0% post-intervention (p=0.008). Although not statistically significant, overall 3-hour and 6-hour bundle compliance increased from 89.1% and 70.0% pre-intervention to 95.2% and 83.8% post-intervention (p=0.524, p=0.101), respectively. See figure 4 for further details regarding each component.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bundle compliance pre and post quality improvement implementation. Patients with CMS discharge diagnoses of ‘severe sepsis’ or septic shock with time of identification in the ED grouped by pre-intervention (orange; 1 September 2019 to 31 May 2020) and post-intervention (blue; 1 June 2020 to 31 December 2020). Percentage of patients individual SEP-1 metrics (initial lactate, repeat lactate when applicable, blood cultures before antibiotic administration, appropriate antibiotics, intravenous fluid bolus administration (30 cc/kg), vital sign/fluid status reassessment after fluid resuscitation, and vasopressor administration when appropriate), as well as overall 3-hour and 6-hour bundle compliance. CMS, Centers for Medicare and Medicaid Services; ED, emergency department; SEP-1, Severe Sepsis/Septic Shock Early Management Bundle.
Discussion
Standardised care for early identification and time-sensitive treatments initiated in the ED have led to improvements in survival for life-threatening illnesses, including acute myocardial infarction, stroke and trauma.27 Over the past two decades, significant improvements in sepsis research have led to similar bundled care guidelines put forth by the Surviving Sepsis Campaign and adopted by CMS and state level Departments of Health. Compared with acute myocardial infarction and stroke compliance metrics, sepsis compliance has many more components spanning a longer duration of time and requiring frequent reassessments, contributing to higher complexity. Physicians practicing in the ED are tasked with simultaneously providing care to multiple patients with potentially life-threatening illnesses. This makes it difficult for a single provider to ensure capture of all components of sepsis bundled care on a regular basis in a fast-paced, high turnover environment as is the ED. Furthermore, the sepsis bundle components are over 6 hours, unlike other quality metrics, which inherently adds multiple transitions of care among ED providers and from the ED to the inpatient setting, making later portions of the bundle prone to error or misses. Having a system-wide process in place is therefore beneficial for promoting bundle compliance. An EHR tool is a crucial element to this approach as it helps facilitate between the transitions of care to avoid missing sepsis bundle components. However, an EHR tool alone may not be sufficient in increasing sepsis bundle compliance without appropriate integrations into the workflow, implementation strategies and efforts aimed at the workforce. This study adds to the growing breadth of evidence that, when tied to other quality implementation strategies including education, huddles, checklists and provider feedback, there is significant increase in utilisation of an EHR tool and subsequent improvement in sepsis bundle compliance.
In this study, we report increased utilisation of a sepsis EHR tool through a multifaceted quality initiative. While the EHR tool was live at our site since September 2019, its use from September 2019 through May 2020 was just 23.3%. After our intervention, we saw increased use of the EHR tool to 87.2%. This finding highlights the importance of education initiatives and specific training targeted at EHR tool utilisation, which is congruent with findings reported by previous studies.
Use of the EHR tool was significantly associated with increased overall sepsis bundle compliance, as well as with several individual sepsis bundle components as outlined in the results above. The individual bundle components with the largest percentage increase in compliance include administration of 30 cc/kg intravenous fluids, measurement of a second lactate if the initial lactate is ≥2 mmol/L, and vital sign reassessment after fluid resuscitation. Each of these components requires reassessment later in the course of patients with sepsis after the initial resuscitation and are, as such, likely more prone to human error during transitions of care. These bundle components were directly prompted by the EHR tool, which appears to have led to significantly increased likelihood of compliance. Measurement of a second lactate and response to initial therapy is vital for determining the trajectory of patients with sepsis and can help identify patients with more severe illness (eg, lactate that does not clear or increases, persistent hypotension). Earlier identification may aide in triaging patients to an appropriate level of care or starting additional interventions, such as vasopressors. While the association was not significant, we did find that patients in which the EHR tool was used were more likely to receive appropriate vasopressor therapy than those in which the EHR tool was not used.
In the separate cohort of patients coded as severe sepsis or septic shock by ICD-10 discharge codes, 6-hour SEP-1 bundle compliance was 98.6% in patients in whom the EHR tool was used, compared with just 14.2% in patients in whom the tool was not used. Patients with severe sepsis and septic shock have higher mortality compared with those without organ dysfunction and have been shown to have significant mortality benefit from timely antibiotics and early goal-directed therapy.35
Irrespective of EHR tool use, we found a significant increase in 6-hour bundle compliance in the period following the quality initiative in the cohort of patients coded as severe sepsis or septic shock by ICD-10 discharge codes. In this group, 83.8% of patients met 6-hour bundle compliance in the months following the initiative, compared with 70.0% of those in the months beforehand. The effect of targeted sepsis education and feedback seem to increase the likelihood of bundle compliance, while the EHR tool appears to improve quality care and compliance even further.
NYU Langone Hospital—Brooklyn has designated a physician and nursing leadership dyad which is responsible for continuing to provide direct feedback to nurses and providers regarding sepsis case performance. Leadership of the sepsis work group continues to elicit EHR tool feedback from users, resulting in ongoing modification of the tool overtime. Sepsis cases continue to be reviewed by the sepsis work group on a weekly basis, and EHR tool utilisation monitored. Additional recognition and process education is planned when sepsis bundle compliance and EHR tool utilisation fall below a threshold established by the sepsis work group. Through these processes, the approach has proved sustainable to date at our institution.
Limitations
This is a single-centre study with profound support from departmental staff, achieving onboarding of 100% of physicians, nurses and PAs in the ED during the implementation phase. As such, our data may not be representative of other institutions, though several other studies have shown similar success via quality initiatives focused on improving sepsis care.
While usability of our EHR tool was actively evaluated by users, the initial educational materials and methods focused on recognition of sepsis and process education for EHR tool utilisation were not formally evaluated by trainees, which may potentially limit the quality of the initial educational intervention.
Furthermore, during the height of the COVID-19 pandemic, our hospital system as well as other systems nationwide saw a decrease in sepsis bundle compliance and an overall increase in mortality. Some of our retrospective cohort analysis comparing pre-intervention and post-intervention bundle compliance overlaps with the peak of COVID-19 pandemic in New York City, which may contribute to some of the differences observed.
The authors recognise the unique limitations of both populations in this study. The first population—the intention-to-treat population—includes patients with ultimate diagnoses of sepsis, severe sepsis and septic shock as well as patients with suspected sepsis who ultimately had an alternate diagnosis. As such, patients without sepsis may have been initiated on a sepsis protocol. Consequences of inappropriate antibiotic administration, over-resuscitation with intravenous fluids and provider bias have been extensively discussed in previous literature. However, the authors believe that this population most accurately represents the dynamic nature of patient care in the ED, where multiple emergent aetiologies are often simultaneously considered based on a patient’s presentation, and which change over time as more information becomes available. The second population—the population of patients with data submitted to CMS based on inpatient discharge diagnosis codes—fails to capture patients who were miscoded and who were treated for sepsis in the ED with improvement and does not differentiate patients who developed sepsis later during their inpatient stay from those with time of onset in the ED.
Our study does not describe baseline characteristics of patients for whom the EHR tool was and was not used or of patients pre- and post-intervention, and as such, cannot account for confounding variables and is not designed to report on outcome measures, such as mortality. Patient characteristics—including age, comorbidities, illness severity, infection type, among others—may additionally confound differences in bundle compliance reported in this study. We recognise the inherent limitations in process measurements as outcomes, and intend to measure patient-centred metrics in future research.
Conclusion
In this single-centre study, we show the effectiveness of a quality improvement initiative and EHR tool in increasing sepsis bundle compliance for patients presenting with sepsis to the ED. We plan to perform additional analyses on the impact of the EHR tool and compliance on patient centred outcomes. As the SCC guidelines now call for a 1-hour bundle,12 we anticipate several additional barriers to compliance including time from door-to-triage and from triage-to-patient rooming that may impact early identification and treatment of sepsis and envision several other targets in which future initiatives may be directed as CMS reimbursement practices adapt to newer sepsis guidelines.36
Data availability statement
No data are available. No data from this study are available for reuse by other work groups.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to acknowledge all emergency department staff at NYU Langone—Brooklyn for their participation in this effort. We would like to specifically acknowledge Kathy Peterson, and Stephen Stark for supervising nursing education, onboarding and feedback with EHR tool usage; Patricia Abruzzino and Alessia Toscano for data collection and organisation; Kashif Creary for APP education and feedback; Ian Wittman, Nancy Conroy, Kar-Mun Woo and Anup Chitnis for physician education and supervision; and Edwin Pineda, Dave Johnson, and the NYU Langone Medical Center Information Technology team for their development of and collaboration on the Epic EHR tool.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors NMW and CD were responsible for study design, data collection and analysis, primary literature review, intervention, manuscript preparation and critical revision. JRC was responsible for study design, intervention and manuscript review. NT was responsible for data quality assurance, statistical analysis and manuscript review. SM was responsible for study design, intervention and manuscript review. CJ was responsible for study design, intervention, data analysis and manuscript review. All authors approve the final manuscript as submitted. CD is responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.